Introduction
Schwannomas, also known as neurilemomas or neurinomas, are the most common type of benign peripheral nerve sheath tumors (PNSTs) in adults, accounting for approximately 80% of cases [1,2]. These slow-growing, encapsulated tumors originate from Schwann cells and represent between 5% and 8% of all soft tissue tumors [3-5]. While they can affect people of any age, they are most frequently diagnosed in individuals between 20 and 50 years old [2,4].
Typically, schwannomas present as solitary lesions. Multiple tumors are often associated with neurofibromatosis type 1 (NF-1) or type 2 (NF-2), but they can also occur independently of these conditions. When multiple schwannomas appear without manifestations of neurofibromatosis, the condition is referred to as schwannomatosis or neurilemmomatosis, which is now recognized as a distinct clinical entity [6,7].
While schwannomas commonly occur in the head, neck, and upper extremities, involvement of the sciatic nerve is exceptionally rare, accounting for less than 1% of all schwannoma cases [5]. Because of the sciatic nerve's location, these tumors may remain asymptomatic for long periods or present as a palpable mass.
The clinical presentation of multiple sciatic nerve sheath tumors is variable. Chronic pain is the most frequent symptom in patients with schwannomatosis [8]. Other symptoms resulting from nerve compression include radiculopathy, paresthesia (numbness), and motor weakness. Interestingly, the severity of symptoms does not always correlate with tumor size, instead, the anatomical location and degree of neural compression are often more decisive factors [9,10].
Magnetic resonance imaging (MRI) is considered the gold standard for diagnosis, providing crucial information about the tumor's relationship to the nerve. Surgical resection, specifically simple enucleation that preserves the anatomical integrity of the nerve, remains the primary and most effective treatment for both solitary and multiple schwannomas [1,5]. Post-surgical prognosis is generally excellent, with a very low rate of recurrence or malignant transformation, which is estimated at approximately 1% [3,11,12].
Case Presentation
A 33-year-old premenopausal, nulliparous female presented with a left buttock lump and chronic severe pain associated with it, which was also radiating along the entire left lower limb, for the past 5 years. She did not have any comorbidities. Her gluteal swelling and pain were insidious in onset and gradually progressive over time. She did not have a history of prior trauma or major surgery. After obtaining informed consent, all relevant clinical, biochemical, imaging and histopathological evaluations were performed.
Clinically, a 5x5 cm, mobile mass was noted in the left gluteal region, in the muscular plane. Her left lower limb power was ⅘, tone was normal, and sensations were intact. There were no signs of vascular deficit. Her biochemical and hematological parameters were normal. She was evaluated with an MRI of the hips including the left lower limb, which revealed - a well-defined, soft tissue density lesion measuring 5x6x5.9 cm, in the intermuscular plane of the left gluteal region (Figure 1). It was in close relation to the neurovascular bundle, showing altered signal intensity. Similar lesions were noted of size 3.4x3.5x4.9 cm and 2.8x3.5x3.9 cm in the mid-thigh region (Figure 2) - s/o multiple nerve sheath tumors in the left gluteal and intramuscular plane of the left thigh region. Core needle biopsy from the gluteal mass reported benign spindle cell neoplasm, with possibility of neurogenic origin.
She was operated with surgical excision of all three masses. In the gluteal region 6x6 cm soft tissue mass was noted adherent to the sciatic nerve. Two similar soft tissue masses of size 4x3 cm and 3x3 cm were noted along the sciatic nerve in the midthigh region. Sciatic nerve fibres were preserved.
The final histopathology report confirmed all the three masses as schwannoma. There were alternating hypercellular (Antoni A) and hypocellular (Antoni B) areas. Antoni A areas consisted of compact spindle cells with elongated nuclei arranged in fascicles, often exhibiting nuclear palisading and formation of Verocay bodies (Figure 3). Antoni B areas consisted of loosely arranged myxoid stroma along with fewer cells. Focal areas of hemorrhage and perivascular lymphocytic inflammatory infiltrates were noted.
In the immediate postoperative period, her left lower limb power was ⅗, tone was normal, and sensations were intact. She was rehabilitated with the help of a physiotherapist and gradually over a period of two months, she regained complete power in her left lower limb.
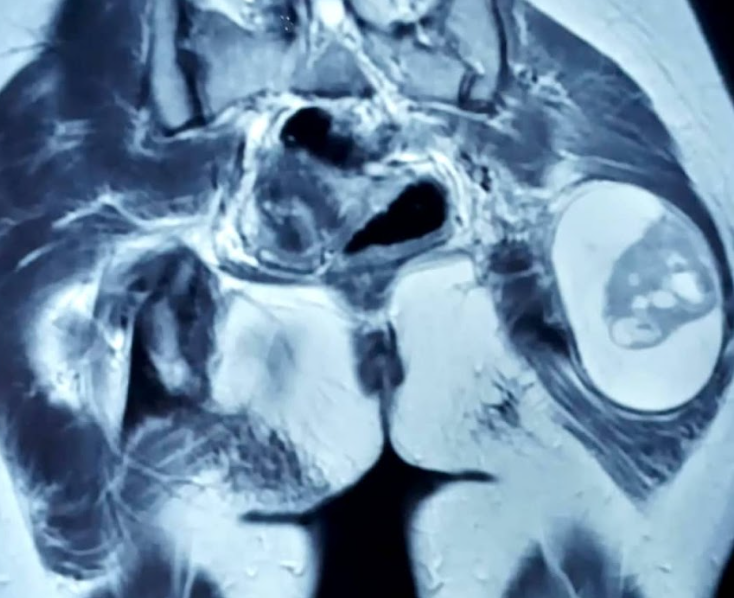
Figure 1.Soft tissue density lesion measuring 5x6x5.9 cm, in the intermuscular plane of the left gluteal region.
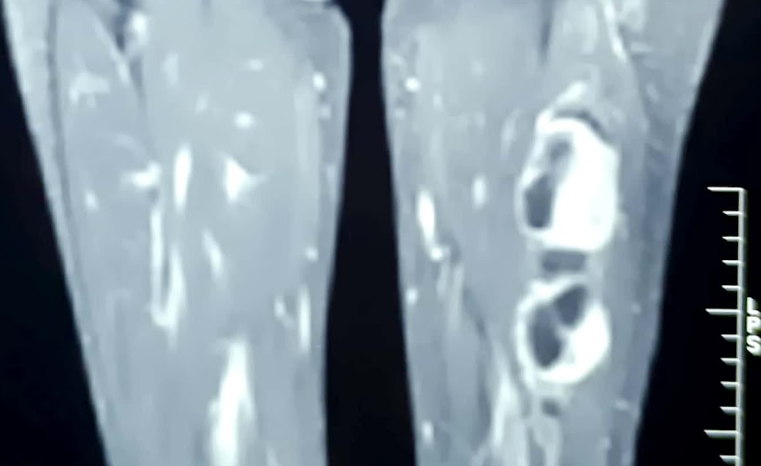
Figure 2. Soft tissue density lesions of size 3.4x3.5x4.9 cm and 2.8x3.5x3.9 cm, in the mid-thigh region.
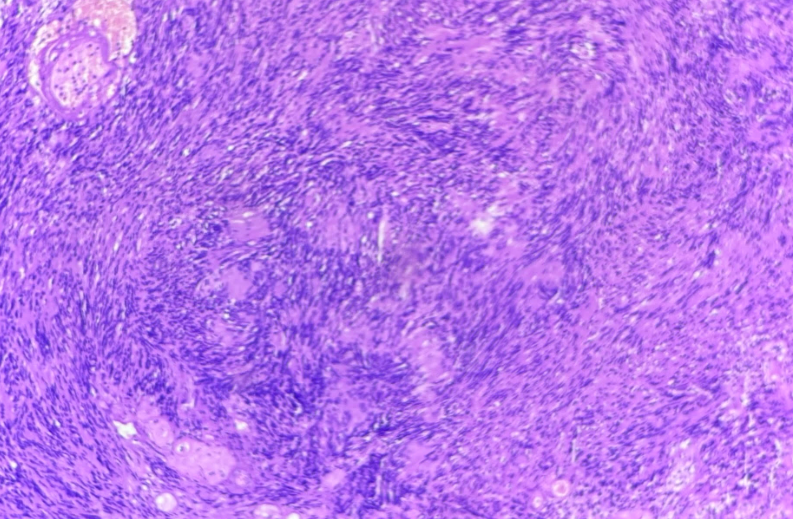
Figure 3. Antoni type A areas, showing compact bundles of spindle cells and Verocay bodies.
Discussion
Schwannomas are the most frequent benign peripheral nerve sheath tumors in adults, originating from Schwann cells [1,2]. While typically solitary, slow-growing, and encapsulated, the presence of multiple tumors within a single nerve, particularly the sciatic nerve, is an exceptionally rare clinical scenario, representing less than 1% of all schwannoma cases [5]. These multifocal presentations are often linked to NF-1 or 2, but they may also manifest as schwannomatosis, a distinct clinicopathological entity defined by multiple schwannomas in the absence of other neurofibromatosis markers like vestibular tumors, café-au-lait spots, or Lisch nodules [6,7]. Our patient did not have any suggestive clinical manifestations of NF-1 or 2, pointing towards the diagnosis of schwannomatosis.
The clinical presentation of sciatic schwannomas is often non-specific, frequently leading to diagnostic delays or misdiagnosis as discogenic sciatica. Patients typically present with chronic pain or a palpable mass, although neurological deficits such as motor weakness or sensory impairments are relatively uncommon unless the tumors reach a substantial size [8]. Our patient presented with a long-standing gluteal mass. It was associated with chronic severe pain. Initially the pain was of low intensity, which gradually progressed to its severe form. The other two masses in the midthigh region were asymptomatic. The anatomical location and the degree of neural compression are often decisive factors for symptoms severity. For instance, giant schwannomas (exceeding 5 cm) can occasionally remain asymptomatic for long periods despite their significant volume [9,10].
MRI remains pivotal for diagnosis, offering characteristic insights such as the "target sign" - a hyperintense peripheral rim with a low-intensity centre on T2-weighted images. MRI also helps distinguish these lesions from neurofibromas by identifying the "split fat sign" or "fascicular sign" [13]. Definitive diagnosis is confirmed via histological examination, which classically reveals a biphasic pattern - Antoni type A areas, characterized by compact bundles of spindle cells and Verocay bodies, and Antoni type B areas, featuring a loose, myxoid matrix [10,13]. Similarly in our patient, there were alternating Antoni A and Antoni B areas. Uniform S-100 immunostaining further differentiates schwannomas from the variable patterns seen in neurofibromatosis [14].
Surgical resection through simple enucleation is the primary treatment, aimed at complete removal while preserving the anatomical and functional integrity of the nerve [1,5]. As schwannomas grow eccentrically and displace rather than infiltrate nerve fascicles, they can usually be dissected away from the parent nerve without causing permanent damage. The use of intraoperative neurophysiological monitoring (INM) is essential, especially in complex or giant cases, to identify functional nerve fibers and minimize the risk of postoperative neurological deficits [15]. In our case, despite unavailability of the INM, all three masses were surgically resected with preservation of the sciatic nerve.
While most patients experience significant pain relief and favorable functional outcomes, the risk of minor postoperative motor or sensory deficits exists, particularly with large or pelvic tumors. The overall prognosis remains excellent, with a very low recurrence rate and a risk of malignant transformation estimated at approximately 1% [11,12].
Although bearing multiple limitations, like lack of immunohistochemistry (IHC) and long term follow up, this case report contributes to the medical literature of schwannomatosis and emphasises on the role of comprehensive imaging and pathology for its definitive diagnosis. Continued research into the genetic and molecular mechanisms of schwannomatosis may further refine future diagnostic and therapeutic strategies.
Conclusion
Multiple sciatic nerve schwannomas represent an exceptionally rare clinical entity, often manifesting as schwannomatosis in the absence of neurofibromatosis. While these slow-growing tumors may remain asymptomatic, they can eventually lead to chronic pain or neurological deficits. MRI and histopathology are crucial for accurate diagnosis and distinguishing these lesions from other nerve sheath tumors. Surgical resection remains the gold standard of treatment, ensuring complete tumor removal while preserving functional nerve integrity. Overall, surgical intervention yields a favorable prognosis with minimal risk of recurrence, highlighting the importance of thorough clinical evaluation.
Declarations
Conflicts of interest
There is no conflict of interest associated with this study.
Consent to participate
There is consent to participate.
Consent for publication
There is consent for the publication of this paper.
Authors' contributions
The authors equally contributed the work.
Funding Statement
No funding sources.