
Pulmonary Cryptococcosis with Disseminated Involvement in Advanced HIV: A Tuberculosis Mimic from a TB-Endemic Region
Authors

##plugins.themes.bootstrap3.article.sidebar##
##plugins.themes.bootstrap3.article.main##
Abstract
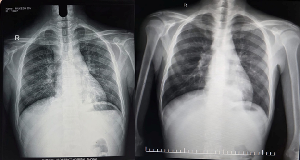
Background: Cryptococcosis is a life-threatening opportunistic fungal infection predominantly affecting individuals with advanced HIV infection. In tuberculosis (TB)-endemic countries, pulmonary and disseminated cryptococcosis may closely resemble TB, resulting in delayed diagnosis and inappropriate therapy. Case Presentation: A 30-year-old man presented with chronic cough, fever, weight loss, diarrhea, and generalized lymphadenopathy. He was newly diagnosed with advanced HIV infection (CD4 count 30 cells/mm³). Imaging revealed mediastinal lymphadenopathy and bilateral consolidations. Sputum potassium hydroxide preparation, supraclavicular lymph node biopsy, bronchoalveolar lavage cytology, and serum cryptococcal antigen testing confirmed disseminated cryptococcosis involving pulmonary, nodal, and ocular sites. Cerebrospinal fluid examination was normal. The patient improved significantly following induction therapy with liposomal amphotericin B plus flucytosine. Conclusion: Disseminated cryptococcosis can closely mimic tuberculosis in high TB-burden settings. Early fungal evaluation and prompt antifungal therapy are critical to reducing morbidity and mortality in advanced HIV infection.
##plugins.themes.bootstrap3.article.details##
Copyright (c) 2026 Palash Agarwal, Abhinav Choubey, Alkesh Khurana, Ujjawal Khurana

This work is licensed under a Creative Commons Attribution 4.0 International License.
Creative Commons License All articles published in Annals of Medicine and Medical Sciences are licensed under a Creative Commons Attribution 4.0 International License.
Abhinav Choubey, Department of Pulmonary Medicine, AIIMS Bhopal, India.
Asst. Professor, Department of Pulmonary Medicine, AIIMS Bhopal, India.
Alkesh Khurana, Department of Pulmonary Medicine, AIIMS Bhopal, India.
Prof and HOD, Department of Pulmonary Medicine, AIIMS Bhopal, India.
[1] Rajasingham R, Smith RM, Park BJ, Jarvis JN, Govender NP, Chiller TM, et al. Global burden of disease of HIV-associated cryptococcal meningitis: an updated analysis. Lancet Infect Dis. 2017;17(8):873–881.
[2] Maziarz EK, Perfect JR. Cryptococcosis. Infect Dis Clin North Am. 2016;30(1):179–206.
[3] Sharma SK, Mohan A. Tuberculosis: from an incurable scourge to a curable disease. J Assoc Physicians India. 2004;52:35–40.
[4] Sloan DJ, Parris V. Cryptococcal meningitis: epidemiology and therapeutic options. Clin Epidemiol. 2014;6:169–182.
[5] Howard-Jones AR, Sparks R, Pham D, Halliday C, Beardsley J, Chen SC. Pulmonary cryptococcosis. J Fungi (Basel). 2022;8(11):1156.
[6] Kawamoto K, Miyoshi H, Suzuki T, et al. Clinicopathological features of cryptococcal lymphadenitis and review of literature. J Clin Exp Hematop. 2017;57(1):26–30.
[7] World Health Organization. Guidelines for diagnosing, preventing and managing cryptococcal disease among adults, adolescents and children living with HIV. Geneva: WHO; 2022.
[8] Perfect JR, Dismukes WE, Dromer F, et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by IDSA. Clin Infect Dis. 2010;50(3):291–322.
[9] Boulware DR, Meya DB, Muzoora C, et al. Timing of antiretroviral therapy after diagnosis of cryptococcal meningitis. N Engl J Med. 2014;370:2487–2498.