
Role of Maternal Serum ɓHCG in Prediction of Early Onset Pre Eclampsia and It’s Correlation with Uterine Artery Doppler
Authors

##plugins.themes.bootstrap3.article.sidebar##
##plugins.themes.bootstrap3.article.main##
Abstract
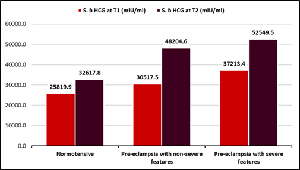
Background: Hypertensive disorders during pregnancy remain amongst the most significant and intriguing unsolved problems in obstetrics. The study aims at testing the hypothesis that women with high Serum beta hCG levels and alternations in waveforms in uterine artery doppler in first and second trimester have high risk of developing pre eclampsia. Methods: Serum ɓ hCG estimation was done by Sandwich chemiluminescence immunoassay method. All uterine artery waveforms were obtained using ultrasound machine attached to a 3.5 MHz curvilinear transducer, with color and pulsed Doppler abilities. Results: The mean maternal Serum ɓ HCG level in non severe pre eclampsia in first and second trimester were 30517.5+-11076.2 and 48204.6+-12074.0 respectively and for severe pre eclampsia were 37213.4+-11968.4and 52549.5+-12074.0 respectively which were significantly greater than normotensive (25819.9+-10017.8 and 32617.8+-6759.0 respectively p value<0.001). The number of complications in preeclampsia group were more than normotensive once. Conclusion: Mean ɓHCG levels are higher in preeclampsia group as compared with normotensive and maternal and fetal complications associated.
##plugins.themes.bootstrap3.article.details##
Copyright (c) 2025 Prof. Shaily Agarwal, MS, Dr Sulfiya Shakeel Siddiqui, Prof. Renu Gupta, MS, Prof. Neena Gupta 1, MS, Dr. Divya Dwivedi, MS, Dr. Ashok Kumar Verma, MD, Dr. Deepak Anand, MD

This work is licensed under a Creative Commons Attribution 4.0 International License.
Creative Commons License All articles published in Annals of Medicine and Medical Sciences are licensed under a Creative Commons Attribution 4.0 International License.
Prof. Shaily Agarwal, MS, Professor, Department of Obstetrics and Gynaecology, Ganesh Shanker Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India.
Professor, Department of Obstetrics and Gynaecology, Ganesh Shanker Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India.
Dr Sulfiya Shakeel Siddiqui, Junior Resident, Department of Obstetrics and Gynaecology, Ganesh Shanker Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India.
Junior Resident, Department of Obstetrics and Gynaecology, Ganesh Shanker Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India.
Prof. Renu Gupta, MS, Professor & Head, Department of Obstetrics and Gynaecology, Ganesh Shanker Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India.
Professor & Head, Department of Obstetrics and Gynaecology, Ganesh Shanker Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India.
Prof. Neena Gupta 1, MS, Professor, Department of Obstetrics and Gynaecology, Ganesh Shanker Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India.
Professor, Department of Obstetrics and Gynaecology, Ganesh Shanker Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India.
Dr. Divya Dwivedi, MS, Professor, Department of Obstetrics and Gynaecology, Ganesh Shanker Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India.
Professor, Department of Obstetrics and Gynaecology, Ganesh Shanker Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India.
Dr. Ashok Kumar Verma, MD, Professor, Department of Radiology, Ganesh Shanker Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India.
Professor, Department of Radiology, Ganesh Shanker Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India.
Dr. Deepak Anand, MD, Associate Professor, Department of Community Medicine, Ganesh Shanker Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India.
Associate Professor, Department of Community Medicine, Ganesh Shanker Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India.
[1] Cunningham, LB, Spong DH, Casey, Sheffield; Hypertensive disorders chapter 40; Williams obstetrics 24th edition, Mc Graw Hill Education, Newyork.
[2] Kaur Gumandeep, Jain Vimla, Mehta Seema, Himani Sunita; Prediction of PIH by Maternal Serum Beta HCG Levels in the Second Trimester (13-20 weeks) of Pregnancy. J Obstet Gynecol India. 2012;62:32-4.
[3] World Health Organization, Make Every Mother and Child Count, World Health Report, 2005, World Health Organization, Geneva, Switzerland; 2005.
[4] Confidential Enquiry into Maternal and Child Health (CEMACH), Perinatal Mortality 2006. England, Wales and Northern Ireland, CEMACH, London, UK; 2008.
[5] L. Dubey, "The global impact of pre-eclampsia and eclampsia," Semi Perinatol. 2009;33:130-7.
[6] Yu CK, Khouri 0, Onwudiwe N, Spiliopoulos Y, Nicolaides KH. Prediction of pre-eclampsia by uterine artery Doppler imaging: relationship to gestational age at delivery and small-for-gestational age. Ultrasound Obstet and Gynecol. 2008;31:310-3.
[7] Witlin AG, Saade GR, Mattar F, Sibai BM. Predictors of neonatal outcome in women with severe preeclampsia or eclampsia between 24 and 33 weeks' gestation. American J Obstet Gynecol. 2000; 182:607-11.
[8] Irgens HU, Roberts JM, Reisæter L, Irgens LM, Lie RT. Long term mortality of mothers and fathers after pre-eclampsia: population-based cohort study Pre-eclampsia and cardiovascular disease later in life: who is at risk? BMJ. 2001;323:1213-7.
[9] P.von Dadelszen, L.A. Magee, and J.M. Roberts, "Subclassification of Preeclampsia," Hypertension Preg. 2003;22:143-8.
[10] Hsu CD, Chan DW, Iriye B, Johnson TR, Hong SF, Repke JT. Elevated serum human chorionic gonadotropin as evidence of secretory response in severe preeclampsia. American J Obstet and Gynecol. 1994;170:1135-8.
[11] Dr. Sangeereni, Dr. A Mallika and Dr. Revathi M: Significance of β-human chorionic gonadotropin in pre eclampsia and normotensive mothers. International Journal of Clinical Obstetrics and Gynaecology 2018; 2(5): 84-87.
[12] Shokry M, Bedaiwy MA, Fathalla MM, Alsemary A, Elwakil S, Murphy A. Maternal serum placental growth factor and soluble fms-like tyrosine kinase 1 as early predictors of preeclampsia. Acta Obstet Gynecol Scand. 2010;89:143-146.
[13] Marek Zygmunt, Friederike Herr, Stefanie Keller-Schoenwetter, Karin Kunzi-Rapp, Karsten Münstedt, C. V. Rao, Uwe Lang, Klaus T. Preissner, Characterization of Human Chorionic Gonadotropin as a Novel Angiogenic Factor, The Journal of Clinical Endocrinology & Metabolism, Volume 87, Issue 11, 1 November 2002, Pages 5290–5296.
[14] Tuffnell DJ, Jankowicz D, Lindow SW, Lyons G, Mason GC, Russell IF, et al. Outcomes of severe pre-eclampsia/eclampsia in Yorkshire 1999/2003. BJOG. 2005;112:875–80.
[15] Vidyabati RK, Hijam D, Singh NK, Singh WG. Serum beta hCG and lipid profile in early second trimester as predictors of pregnancy induced hypertension. J Obstet Gynecol India. 2014;60:44–50.
[16] Towner D, Gandhi S, El Kady D. Obstetric outcomes in women with elevated maternal serum human chorionic gonadotropin. Am J Obstet Gynecol. 2006;194:1676–81. doi: 10.1016/j.ajog.2006.03.011.
[17] Taché V, Baer RJ, Currier RJ, Li CS, Towner D, Waetjen LE, et al. Population-based biomarker screening and the development of severe preeclampsia in california. Am J bstet Gynecol. 2014;211:377e1–8. doi: 10.1016/j.ajog.2014.03.026.
[18] Davidson EJ, Riley SC, Roberts SA, Shearing CH, Groome NP, Martin CW. Maternal serum activin, inhibin, human chorionic gonadotrophin and alpha-fetoprotein as second trimester predictors of pre-eclampsia. BJOG. 2003;110:46–52.
[19] Jiji DB. Cabading ML., Benjamin BA. A Comparative Study to Find the Maternal and Foetal Outcome among Pregnancy Induced Hypertension and Non-Pregnancy Induced Hypertension Gravid Women. Scholars. J Applied Med Sci. 2014;2(4):1286-9.
[20] National high blood pressure education Program working group, report on high blood pressure in Pregnancy. American J Obstetrics Gynecol. 1990;163:1691-712.
[21] Patel Ravikant. BarialHinal, Patel Hinaben Tab A Nava Sunil; "A study on pregnancy induced hypertension and foetal outcome among patient with PIH at tertiary care hospital, Valsad"; International Journal of Community Medicine and Public Health; Patel R et al. Int J Community Med Public Health. 2017 Nov:4(11):4277-4281, DOI: http://dx.doi.org/10.18203/2394-6040.1jcmph20174843.
[22] Heikkila A, et al. Elevated Maternal Serum HCG in The Second Trimester Increases Prematurity Rate and Need for Neonatal Intensive Care in Primiparous Pre Eclamptic Pregnancies, Hypertens Pregnancy, 2001.
[23] Harrington K, Campbells S. Fetal size and growth. Curr Opin Obstet Gynecol. 1993; 5:186-94.